

May 28, 2021
Dear Interested Readers,
Hope Needs A Plan: Moving Upstream From Quality, Safety, and the Triple Aim
About three paragraphs from the end of the main section of last Friday’s Healthcare Musings I wrote:
Since we have not had the will to discard fee for service payment in favor of some form of universal capitation for the care of the population, we have tried to go forward with the improvement of our care system through bonuses and penalties based on patient satisfaction and quality and safety metrics. I fear, and the pandemic suggests, that we have not accomplished much. This pandemic has revealed that twenty years of focus on quality and safety did not prepare us for the domestic, not to mention the worldwide, challenge COVID presented. Some of the economic and individual devastations of the pandemic might have been avoided if we had truly operationalized the suggestions in Crossing the Quality Chasm which was really a strategic plan that never got adequate focus, acceptance, or traction within healthcare and within the political process that determines the rules and finance of care delivery.
I hope that did not sound like I was depressed. It was a realistic appraisal of the results of a grand effort of twenty years.
Looking back twenty and twenty-five years, the quality and safety movement as summarized in Crossing the Quality Chasm (2001) and the evolution of the Triple Aim (2008) could be viewed as one huge “Lean like” experiment. For review, the big step forward in Crossing the Quality Chasm was the realization that true quality healthcare had six “domains” that were: Patient centeredness, Safety, Equity, Efficiency, Effectiveness, and Timeliness. The combination of those parameters produced care that would cost less and yield better outcomes through the appropriate and timely provision of care and good stewardship of resources. The authors were explicit about the fact that good primary care and preventive care were essential and that the best finance mechanism would be value-based, and most likely some form of capitation with risk-sharing.
The Triple Aim affirmed the conclusions and recommendations of Crossing the Quality Chasm and emphasized expanding the benefits to everyone through attention to the health of the community and universal access to care. The hypothesis of the experiment that we have in essence been testing was: If we focus on the six domains of quality and extend the benefit to everyone in the community we will be able to continuously improve the health of the community while controlling the cost of care to sustainable levels and simultaneously giving everyone the personalized care they desire.
Well, we failed. We never really tested the hypothesis. Fee for service practice with its predilection for overuse, misuse, and underuse of appropriate care is still the primary form of finance. Twenty years later the cost of care relative to GDP is more than ever before, death and disability from medical errors are greater than ever, our longevity and almost every other metric put us in last place compared with our peer nations. In some areas like maternal and child health, and infant mortality we are behind places most of us would never consider living. We were able to continue the universal misconception that we really knew what we were doing until the pandemic gave our deficiencies no place to hide. If the last twenty years had been a Lean project we would have to recognize that we had not achieved our objective as described by the Triple Aim. In Lean thinking, failure is an opportunity to learn. The next step is to reflect on why we failed and develop a new hypothesis that is built on what we have learned and then try again.
The need for a new approach is appreciated by some people who are not currently in healthcare. My letter last Friday crossed in cyberspace with a note from an interested reader who is a retired attorney and was once my patient who now lives in Florida. He sent me his thoughts before he read last week’s letter, and I wrote the letter before I got his email. It seems that his conclusions fit with my dark pronouncement of failure. He said:
…I’ve been following your writings on the triple aims and am impressed with the goals and the arguments for them. I’m hoping that Biden pushes hard on advancing the ACA and in the process gets to make at least some of the changes necessary to improve the health care system. My observation is that the existing institutions do a great many things well, including building wonderful facilities, but when they try to change the way physicians practice medicine or the way they are compensated, they hit a stone wall – they are figuratively treading on sacred soil. I think it will take a force outside the institutions to move things, namely the state and federal governments and/or an informed and energized public. The only issues I have heard consistently raised on behalf of the public are more health care coverage for uninsured or ill insured persons and cheaper drug prices. Outside the medical community, I have never heard a discussion of issues such as capitation or the effect on the poor and minorities of failure to have medical coverage. Although the public seems quite aware of some problems, such as hospital infections, I have heard no one insisting that something be done or questioning whether the US experience is better or worse than other wealthy countries. I was fortunate in not being subject to the vicissitudes of our health care system because I joined the Harvard health plan around 1969 or 1970 and stayed in it until a few years ago when we moved to Florida full time. That whole time my family and I received first-class care with no fuss or bother-something most others did not…
That is a message worth considering. As an informed consumer he has come to the same conclusion that I have reached. Simply this, quality, safety, and the Triple Aim are not winning the day. They are laudable objectives, but we’re not really making progress toward them. Even as we have informed people that their care is expensive, ineffective, and likely to be even more expensive in the future while becoming no more effective or available has not made a difference. What is an even greater concern is that the message has not gained effective traction with those of us who deliver care. At the level of a gross and unfair generalization that ignores valiant efforts by a committed minority, we seem much more concerned with the quality of our work lives and the short-term financial durability of our institutions than the results we produce for our patients or the cost of the care we provide.
In a good Lean process when a hypothesis fails to solve the problem we go back to the drawing board where we begin the process of developing a new hypothesis to test because the original problem usually still exists. One thing we try not to do is “to jump to a solution.” My friend and former patient is a lawyer and not a quality improvement consultant so I will forgive him for jumping to the conclusion that “I think it will take a force outside the institutions to move things, namely the state and federal governments and/or an informed and energized public.” He may be right but there are alternative approaches. Sometimes in an improvement process, we realize that we can’t solve the problem that we are looking at without going “upstream” and correcting the origin of the problem that is our concern.
What is upstream from quality, safety, and the Triple Aim? My sense is that our failure is at the confluence of several streams. We need to go upstream in at least three areas. First, the culture of healthcare is a big problem that is getting worse. That is the thesis in Dr. Robert Pearl’s new book, Uncaring: How the Culture of Medicine Kills Doctors & Patients. I just received my copy of the book this week and you can be sure that I will be transferring some of Dr. Pearl’s thoughts to you in subsequent weeks. Second, there is the problem of poverty in America which itself is downstream from several persistent issues. Together the contributors to poverty are essentially the same or closely related to what we label as the ” healthcare disparities.” Finally, there is racism.
As I was thinking that our failure to achieve the Triple Aim is downstream from the internal culture of healthcare and the persistent issues of inequity that create poverty it occurred to me that Pittsburgh is a good metaphor. Pittsburgh sits at the confluence of the Susquehanna and Monongahela Rivers where they join to form the Ohio River. When I Googled Pittsburg I discovered that my metaphor was even better than I realized because there is a hidden underground river that also joins the Susquehanna and Monongahela to help form the Ohio which seems to me like the impact of racism on what we are trying to accomplish. Racism is often underground, discounted, or ignored for its impact on why there is a reluctance for things to change. There is a disturbing movement in many states to outlaw diversity training in schools and the workplace and to make it impossible for subjects like critical race theory to be taught or even discussed in the public schools or state universities. it seems there is a consensus on the right to deny the fact that race has been a factor in our past and continues to be an impediment at the moment and that our past and present are likely to curse our future.
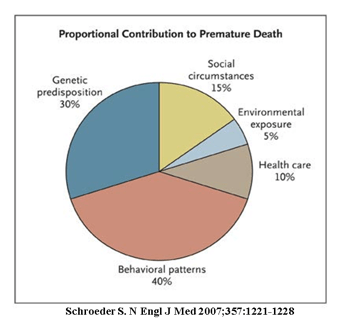
My first reaction to Elizabeth Warren’s recent book Persist was my surprise that she spent so little time writing about healthcare reform. As I read her passionate discussions of our need to invest in childcare, education, public housing, and the differential impact of climate change on the poor, I realized that she was talking about healthcare. She had either by plan or by instinct moved upstream from talking about healthcare the way we have ineffectively talked about it for the last quarter-century to engage in a forceful discussion complete with corrective plans of action for the things that are more powerful origins of disease and disability than can be corrected in our hospitals and ambulatory medical offices. In 2007 Stephen Schroeder published an important description of the origin of premature death. I have used the graphic before but the message it presents is worth review. It suggests that social and environmental factors are huge contributors to the health of the public.
Warren is dedicated to improving healthcare. In her book she says:
I have studied our country’s health-care problem for a long time, and for years I have thought we should do three things: improve the Affordable Care Act; lower drug costs; and move toward full health-care coverage for everyone.
She did not say we should focus on the Triple Aim. I think she knows what my former patient knows, that the language of quality, safety, and the Triple Aim is language that the public doesn’t know and that most of healthcare pays only lip service to with no intention of ever implementing any change that might cause them to become realities. I lifted another quote from her last week. A little further on in the same chapter she writes about her motivation during the presidential primary campaign:
When I decided to get in the race [for the nomination], I was ready to slug it out over every health-care issue on the table. I was eager to talk about how to reduce the cost of insulin and EpiPens. I was prepared to explain how to make unions whole by requiring employers switching to Medicare for All to put the now eliminated cost of health benefits into higher salaries for union workers. I was happy to debate whether we should change our health-care system by taking a couple of big steps or a lot of small steps. And start to finish, I was ready to fight for the ultimate goal of getting universal coverage for all Americans.
Well, she did not win and some might argue that her focus on the importance of universal coverage through something like Medicare for All might have cost her a critical number of votes. What she has done since the primary process has been to continue to focus on the component issues that exist in our society that do impact the health of the nation and its future with or without access to care. Personal economics does make a huge difference in individual health and longevity. During the campaign, Warren developed a multitude of plans to attack the inequities and challenges that face the poor among us. She says that there were eighty-one plans. I believe her. I also believe that if we adopted the bulk of those plans and the transfers of wealth that she proposed to fund them we would go a long way toward reducing healthcare disparities and the cost of improving the nation’s health. We would also be less vulnerable to the next pandemic. She sees it as “national defense.” She says:
Providing a common defense is—or should be—as much about protecting our citizens’ health as it is about protecting us from terrorists or hostile foreign governments.
In her discussion of the importance of “plans” she speaks about our need to address racism:
Sure, we need plans to keep our country safe. We desperately need plans to deal with terrorist threats. But we need more. We need plans to combat systemic racism. We need plans to expand opportunity for all of our children…
She did not win. Joe Biden won, but I think she may have great satisfaction in seeing many of her plans reflected in Biden’s proposed American Jobs Act and his American Families Act. If most of the proposals contained in those pieces of legislation are eventually passed, we will have made huge progress in the struggle to improve the social determinants of health, and we will have done a lot to reduce healthcare disparities.
I close with a return to the letter I got. I have bolded one of the most important things the writer said:
My observation is that the existing institutions do a great many things well, including building wonderful facilities, but when they try to change the way physicians practice medicine or the way they are compensated, they hit a stone wall – they are figuratively treading on sacred soil. I think it will take a force outside the institutions to move things, namely the state and federal governments and/or an informed and energized public.
Between 2008 and 2013, I think that I annoyed a lot of people who were in leadership positions in healthcare in Massachusetts because in speeches, meetings, and in these letters I bemoaned our failure to take institutional responsibility for the high cost of healthcare in our state. I would say that we were the most expensive place in the universe to get care. We were definitely the most expensive state in the most expensive country in the world. I had great hope between 2006 and 2012 that the state was going to be that force outside of healthcare that demanded change and transformation. I would say to whomever might be listening that the series of healthcare laws the legislature was passing was the voice of the public being amplified like a megaphone through the legislature. Some change did occur but the establishment has absorbed the blows and a decade later things have not changed much. Sure a few mergers have been blocked and the state enjoys the lowest uninsured rate in the nation, but the cost of care is still high and the quality is unevenly distributed so that life expectancy in Massachusetts still varies by ZIP code despite great efforts.
I am not sure if we can ever change the culture and practice of medicine from within, and the experience in Massachusetts and with the ACA suggests that it is not much easier to make a change from the outside using the power of government. What hasn’t been a success that deserves more effort is the concerted demands of an educated public. I wish someone would organize Mother’s Against the Inequities and High Costs of Healthcare. Until that happens I am all for seeing what we can accomplish by giving some of Elizabeth Warren’s plans a chance to become law. “Hope needs a plan” and I don’t know of any plans that are more “shovel ready” than the plans she has produced. We may not ever reduce the total cost of care, but I am not ready to say that we can’t improve the social determinants of health.
Sitting On The Dock At Sunset Once Again
One of the saddest days of the year for me is when the local dock service comes by shortly after the Columbus Day weekend and tows our dock and swim platform away for winter storage. I know then that winter is upon us and most outdoor activities for the next six or seven months will require a coat, a hat, and gloves. One of the brightest days of the year is when the same fellows return my dock and swim platform in late May. The return of the dock signals the beginning of summer and means that most hours of the day for the next four months I will be outside and lightly clad.
The dock has several functions. It is where my boats and the boat of one of my neighbors sit when not in use. My grandchildren have literally caught hundreds of sunfish off the end of the dock. The records are about forty-five in an hour and about fifteen on one worm! That much action keeps a granddad busy baiting hooks and taking fish off of hooks. I have also caught a five-pound, twenty-one-inch largemouth bass from the end of the dock while sitting in a rocker and calling into a board meeting. Since the dock is only a few steps from the deck, I often go there when I have only a few minutes to fish.
The dock is a great place to sit in the evening with my wife or some friends to just chat, but best of all it is a great place to sit alone and soak in the peace and tranquility of a lovely late spring or summer evening. The hues of blue and pink in the sky are reflected in the still water. All seems at peace. It is easy to be there and forget one’s worries and the larger collective issues and concerns we face together.
We will be sitting on the dock alone this weekend since most of our usual visitors are traveling for visits and events elsewhere. If you happen to find yourself on Interstate 89 between Concord and Vermont, do stop by. You could catch a few sunfish, maybe even a big bass, and watch the sun go down. The weather prediction is for only occasional showers and temps in the high sixties to low seventies. It should be nice!
Whatever you do, have a happy Memorial Day and enjoy the first weekend of summer.
Be well,
Gene
