

I have been thinking a lot about the future lately. Years ago I concocted a quote that works for me by leaving out a few unnecessary words from a passage in The Age of Unreason by the British business guru and futurist, Charles Handy.
The future we predict today is not inevitable. We can influence it, if we know what we want it to be…We can and should be in charge of our own destinies in a time of change.
Our biggest problem is not our inability to imagine a better future. Atul Gawande has famously said that our problem is not our collective ignorance but rather it is our collective ineptitude. We seem to be unable to collectively execute a strategy for the future. The biggest barrier to that exercise seems to be the self interest that trap us in the problems of the status quo. To imagine and accomplish a better future requires that together we manage our fears, self interests and variations in opinion to achieve the future and the outcomes that we say we jointly embrace.
It is easy to plan and hard to execute the future that we want. Even though we may be experienced, gifted, strong, rational and committed, there is an uncertainty about the future that can trump all of those assets, positive character traits, and competencies. What we often forget as we reassure ourselves about our internal capabilities is that those skills must be aligned against the challenges of a future where there are potent forces that may be moving in a way that will create unforeseen conflict or problematic circumstances.
Those outside forces are a combination of externalities that arise from the will of others as well as from chance and circumstance beyond our control. Sometimes by fate or design, our skills, chance and externalities align and delight us, but the denominator of the frequency of our efforts is much greater than the numerator of our successes.
Pessimism accepted and put aside, let no one ever accuse me of failing to make plans for a better future. I am and have always been a willing conspirator for a better world grounded in the greatest good. The issue has always been how the greatest good is determined. My response to the knowledge that there are external forces and flows that may sweep me toward a future that I want to avoid is to try harder to understand and counter those facts and forces with effective strategies and seek alliances with like minded souls. Experience and others advise me that we must do more than wish or hope for a better future. How do we follow Handy’s advice and begin to “influence the future”? How do we attempt to make the future what we want it to be?
Having set the objective of preparing for a better future, how do we prepare to achieve that objective? Said simply the question is, “What might I do to change the outcome from what will happen if I do nothing?”. A key strategic consideration is, “ How do we build a coalition for the better future that we desire?” This question must be balanced by the age old advice from the Hippocratic Oath, primum non nocere. I prefer to translate this concept of “first do no harm” into something more personal—“If you can’t make it better, please don’t make it worse”.
Lean has taught me a lot about the search for a better future, which is usually, but not always, the search for solutions to current and future problems. In box one of an A3 we have a “reason for action”, an opportunity, concern or problem that needs improvement as we move into the future. We use a process to search for solutions in the future that will lead to an improved state. That search requires creating a catalog of all the issues in the “current state” that contribute to the “reason for action”. That list is composed of barriers, needed changes, or new assets that we must acquire if the target or ideal state is to be achieved in the future. In those searches it is very easy to consider all those factors outside yourself when the only factors over which you theoretically have total control are those that are the answers to the questions, “What part of the problem am I?” and “What can I do to improve the future?”
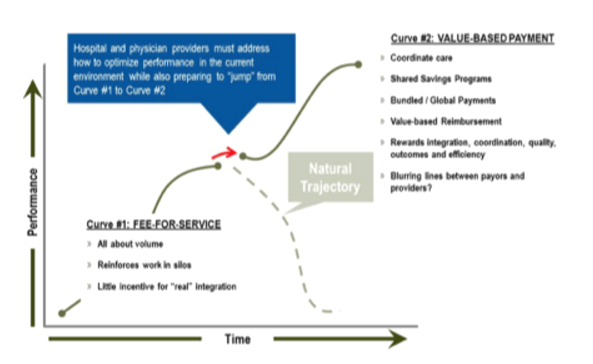
My thoughts about the future have been heightened by the fact that I have recently participated in an exercise with about thirty other people who are interested in the future. We played out various scenarios that may be part of plausible futures in healthcare. These exercises have some similarity to the work described in The Art of the Long View by Peter Schwartz. The exercise was much like the one that I described recently that the Atrius leadership put itself through in early 2009. The idea is to use simulations of what might happen to look for common threads that might generally apply as good strategy or good policy in the future. The elusive goal of the exercise is the Triple Aim. The hope of the exercise is that by “role playing” the potential concerns and objectives of the players in specific markets, the exercise might surface concerns that need further consideration and help us avoid failure in the future by anticipating and preparing for hidden contingencies as we try to move from “volume to value”.
Many healthcare enterprises seem frozen by the ambiguity associated with switching from the fee for service revenue streams that they know so well to the vagaries of “value based reimbursement” or reimbursement for the care of a population. Beyond the uncertainty about whether the new payment mechanism will provide adequate revenue, there is also the realistic understanding that there will be the need to bear more financial risk. The sum of these realities has caused the healthcare economist, Michael Chernow, to say:
“They feel like they are standing with one foot on a sinking dock and the other foot in a tippy canoe”.
There are a host of future considerations and fears that quickly come to mind as we anticipate traveling the road from “volume to value”. To use a worn out cliche, many of us are like deer in the headlights, not knowing what to do first or which way to run to even begin our transition to what has been called “the second curve”. For many this apprehension and uncertainty has created a reluctance to get started with the transformation process even though MACRA is a year old and CMS has recently published its first request for comments on its “rule”.
I think that Jeff Goldsmith was tapping into an undercurrent of fear and resistance in his recent speech at GPIN when he asked the question,
“What if the crowd [healthcare policy wonks and self styled experts] are wrong?”
I will paraphrase the six areas where Jeff wondered if the conventional wisdom offered by the experts about the future might be wrong.
- Are costs really rising uncontrollably and to control them do we really need to change how health providers are paid? He says the cost curve has been bent.
- Is population-based payment the end state of US healthcare payment? He says fee for service will be the foundation of reimbursement for a long time.
- Should providers have to shift from treatment to prevention to manage population health risk? He is not so sure. We have enormous investments in “treatment”.
- Are “disruptive technologies” really going to undermine the traditional business of healthcare, forcing transformative change? He looks at history and quotes Drucker to support an argument that this is an allusion.
- Will consumer empowerment strengthen the role of consumer choice in the health system? -That would be nice but it has not happened yet.
- Will the process of systems mergers and integration that seems to be happening everywhere create new value? Jeff suggests that historically system integration seems more often than not lead to “market power” and increased costs.
He is clever and put up convincing arguments. His position would cause many to question whether or not we are seeing the future clearly. Jeff’s words may have caused some to say to themselves, “If what he is saying is true, why do we need to contemplate so much change in the future? Things are not so bad for me or my patients. My biggest hassles come from the government and the payers with all their rules and regs. I just want to take care of my patients. Perhaps if we just got back to the business of being great in the ways we have always succeeded in taking care of our patients our problems will go away.”
What I heard in Jeff’s message was that the future is not so simple. It is easy to just say reduce the cost of care and pay doctors for value and not volume. It is hard work to prepare for population based payment in the future. What does it mean to change the focus of care from repair to prevention? Do we really think that apps will effectively manage our patients or guide them to better care in a way that will reduce their need for the current system of care? Will our patients become informed at a level that they will be consumers who seek to manage the cost of their care? Will giving up clinical autonomy to a larger system be good for practices or patients?
Any change is hard while you are simultaneously taking care of today’s business. The future will be a function of both what we should do, what we can do, what we are forced to do. Plans for success of the new reimbursement models will be discounted by those who are not so sure change is necessary and attempt to cling to the status quo.
I was not surprised by Jeff’s suggestion that in the future we should return to our roots and focus on what it means to practice. That suggestion is not in conflict with change for the future but it is simplistic because practicing as we have always practiced will not achieve the Triple Aim. Short term, there is validity to his suggestions and the set of current actions that he advises would be a good place for everyone to start their journey from volume to value. He wisely advises:
- Learn to Run on Regular Gas (I assume this means reduce waste and make value based decisions)
- Develop a Fault-Intolerant Clinical Culture Built on Continuous Care Improvement (I agree that a focus on the nuts and bolts of care that is founded on systems thinking will improve safety and outcomes. This means “be Lean” to me.)
- Teach Your Young Clinicians Elegant Diagnosis and Resource Sensitive Clinical Care (Critical thinking and choosing wisely what is necessary and avoiding what adds no value are subjects that need more than lip service)
- Smooth and Light the Patient’s Pathway through the Care Episode (Amen!)
- Become the Health System of Choice in Your Communities and Regions (This is the core of success in a value based system that accepts risk.)
One thing that I know for sure about the future is that debates about what should be done and its urgency will continue. Self interest will remain a consideration, if not a barrier. We will not achieve exactly what we dreamed of with each new initiative. I also know that each time we try and fail, or succeed but not as spectacularly as we had dreamed, we are still getting closer to
Care better than we have ever seen, health better than we have ever known, cost we can all afford, …for every person, every time…
