
One of my occasional delights over the past few years has been to have a friend or former colleague whom I have admired and learned from send me a manuscript or a recently published book that they have written. I am always a little apprehensive when what has been written is already a book. I find myself thinking as I open the package, “What if it is not a good book?” What will I say?” I reason that if what I am presented is a manuscript, there is a chance to offer suggestions that could contribute to the publication. If the book is already in print, any suggestions would have to wait until the second edition! So far I have been lucky with the books. They have needed no input from me!
I have been looking forward to reading Zeev Neuwirth’s new book, Reframing Healthcare: A Roadmap For Disruptive Change, since last February when he announced on his popular podcast, “Creating a New Healthcare” that he had a book coming out in April. Zeev’s podcast has become very popular over the last year and a half. There have been more than 100,000 downloads. If you are not a regular listener, you are missing out on an important opportunity. Each podcast is an in-depth interview and discussion with a disruptive and innovative healthcare leader. In these notes I have directly referenced conversations from the podcasts that Zeev has had with Don Berwick, Eric Topol, and Jeff Thompson.
Zeev’s podcasts have offered me new insights, and have provided me with inspiration that has fueled my own thoughts, and have broadened my understanding of what is possible in the future. I have found his new book to be everything that I hoped it would be and more. It is a must read for any person who cares about the future of healthcare in America and realizes that despite our best efforts we seem to be spinning our wheels and not making much progress.
Before going further let me backup and give you a picture of my experience with Zeev. I first met Zeev in 2005 when Harvard Vanguard hired him to be the Chief of Internal Medicine at our Kenmore Square practice site. Kenmore is the oldest and largest site at Atrius Health. I practiced both Internal Medicine and Cardiology at Kenmore for thirty eight years. At the time Zeev joined us, I was both a practitioner and the chairman of the board. Zeev was fresh from earning his MPH from Harvard’s T.H. Chan School of Public Health. Prior to earning his MPH from Harvard, Zeev had extensive hospital practice and teaching experience at Lenox Hill in New York, and had spent some time in consulting.
Over the years Harvard Community Health Plan, and it’s legacy practices at Harvard Vanguard and Atrius Health, hired some amazing physicians into leadership positions. It did not take me long to realize that Zeev was exceptional and offered something that I had never experienced before in any other colleague or leader. I had never met anyone with more passion for practice, more respect for every member of the clinical team, more focus on the patient, or more ability to search the wider world for the “next new thing” than Zeev brought to work every day.
At the time Zeev was hired our Kenmore practice was struggling. Zeev immediately infused it with energy by bringing us systems improvements through Lean. The support staff loved his leadership and attention to the things that made their work more onerous. Our clinicians recognized that their lives were improved by the efficiencies his methods fostered. Our patients were surprised by the palpable improvements in their care experience. Within a year it was clear that we needed Zeev’s energy and creativity to be applied across all of the fourteen sites of our entire practice. I introduced him to our new CEO and recommended that she give him organizational wide responsibilities, and she appointed him to be our Vice President of Clinical Effectiveness and Innovation. In early 2008 I joined Zeev on the Senior Management Team and tried to enhance his ability to help us by enhancing his title to Chief of Clinical Effectiveness and Innovation. Our offices were separated by just a few steps, and I spent many happy hours sitting in front of his whiteboard which was always covered with ideas that he wanted me to hear that added to my knowledge and gave us new opportunities to explore.
Over the next three and a half years I leaned heavily on Zeev’s strategic thinking, his ability to communicate with everyone in the practice, and his ability to bring new ideas from the outside world into our practice as creative solutions to long standing frustrations. There is no way that I can easily impart to you the impact that Zeev had on our practice, and on me. Theoretically, and according to our org chart, I was his supervisor. In reality the flow was usually the other way around. I was sustained by his energy and enthusiasm, and was constantly learning from him. One fond memory is the day that he got John Toussaint at ThedaCare on the phone to help convince me that we needed to make an organization wide investment in Lean transformation.
Bringing Lean to us was huge, but equally important and perhaps an even greater contribution was his establishment of an extensive leadership academy with a faculty that drew from internal expertise and external experts. I am convinced it was better than any executive training program that was offered by the academic institutions in the Boston area. New professional bonds were developed between managers and leaders from across the practice. Those connections and the common vocabulary developed within the academy then translated into better coordinated performance in our practice. Over four years Zeev was the creator, sustainer, and heart and soul, of this vigorously demanding academy that enhanced the management and leaderships skills of over one hundred graduates. I tell you these things to reenforce Zeev’s position as a person whose opinions and thoughts deserve your attention and consideration.
I was flooded with all these memories of Zeev as I opened his book and began to read. I was immediately rewarded. I have told you about many books. I love books like Elisabeth Rosenthal’s An American Sickness, and Robert Pearl’s Mistreated. Both of those books and many other healthcare articles in newspapers, academic journals, and the “throw away” online medical literature spend much of their energy and print describing the “current state.” In the end they offer some suggestions about how to “fix” what is wrong with our healthcare, but the solutions they offer always seem inadequate compared to the challenges they describe.
Zeev spends very little time talking about a fix of what is broken. He is not interested in a “brownfield” approach to healthcare. He advocates searching for new methods and deeper understanding as we “reframe” our approach to promoting health and aligning healthcare with the Triple Aim. Almost ten years ago Jim Champy, a business writer who had become famous in the nineties with Reengineering the Corporation: A Manifesto for Business Revolution, decided to bring his approach to healthcare and produced a book called Reengineering Health Care: A Manifesto for Radically Rethinking the Delivery of Care. To write the book Champy interviewed Zeev and relied heavily on his thoughts and insights at the time. Zeev has tried as hard as anyone I know to fix what is broken, and now he can tell us with the confidence of a man who has spent great effort to fix what resists fixing that reengineering and simple process improvement won’t get us to the outcomes we desire.
In the splendid essay that forms the introduction to his book, Zeev describes the conviction that has come to him after years of trying to lead efforts fix what is broken. He had the courage to admit that we have been going about the business of improving healthcare all wrong. We can’t get very far “fixing” what is so fundamentally and deeply flawed in its structure and systems as healthcare is today using the same concepts that we used to construct the flawed system. Zeev explicitly describes the two origins of his motivation. He is motivated to meet the needs of patients, and to help those who do the work. He has great respect and concern for healthcare professionals who do their best every day to provide care while working in systems that do not work and are resistant to improvement.
In the second chapter he takes us to the moment in a meeting of senior managers, about three years ago, when he could no longer avoid the feeling that things were not going to get better unless we took a new approach. It was a meeting like so many meetings that we all have attended. He writes:
As I participated in that particular meeting three years ago, I noticed a growing unease welling up inside me—a mix of frustration and déjà vu. The feeling that I had done this all before was overwhelming. “Wait a minute,” I thought to myself, trying to understand the intense emotionality of the moment. “Haven’t I been in this meeting before?” Just like that, I flashed back to a meeting I’d been in five years prior—none of the same people, but the same white coats and suits sitting around the table discussing the same exact topic. What made it viscerally uncomfortable was that it was almost the exact same conversation. We were recirculating the same problems and eerily similar solutions that had been discussed and implemented years before. A moment later, I was flooded with memories of meetings spanning at least a decade and a half—all of them focused on the issues of access and productivity, quality and efficiency. It felt just like Bill Murray made it look like in Groundhog Day; waking up each morning only to find that you’re repeating the same day and series of events over and over again. It was my first—but, unfortunately, not my last—frustrating recognition of the “Groundhog Day” moment in healthcare; a moment we have been caught up in for decades.”
Zeev has concluded that we must have the courage and insight to recognize that we are on the wrong road, or to use his analogy, caught in a series of “groundhog days.” He offers guidance to anyone who accepts the conclusion that the time has come for a reframing. If you are beginning a difficult journey, a road map and travel guide from an experienced traveler of the same road is a welcome asset. Doing better what is not working will not lead to the outcomes that we need, but heading down a new path is a challenge. Despite the dilemma of choosing to stay the course or follow a new road, until we “reframe” healthcare we will continue to see little progress despite our sincere efforts. Reframing means looking at old concerns in new ways. Zeev believes that the process of reframing has already begun. He is observing the reframing process in action. The conversations on his podcast are reports from the innovators and disruptors who are doing the work. The roadmap that he offers to those willing to listen is not an invention or a proposal of something that might be. It is a description of the pieces of the future that are already here and can be seen by those willing to look. He sums up his insight by describing,
“…the steps we need to take in order to assure that we transform the current approach into one that is consumer-centric, community-oriented, value-laden, and sustainable for our children and grandchildren.”
Since Zeev has tried as hard as anyone I know to “re engineer” healthcare, I must listen to him if he contends that we are going about the job in a way that he fears will never get us to the outcomes that we need. His “reframe roadmap” deserves your attention. He also hopes that if you are not in a senior leadership position that you will bring the book’s ideas to the attention of those who do hold power and influence where you work. I know that what Zeev wants you to do is something that he has done himself. He has demonstrated the courage to speak “up” and lead from below. When I was his “boss,” he pushed me to do things that I would never have had the wisdom to do without the benefit of his insights, energy, and persistence. If you have twelve minutes to spare, you can hear Zeev describe his motivations, and his book to Scott Becker. If you listen you will hear him describe his frustration with the search for “magic bullets” that will fix healthcare. You will also hear him say that we must make healthcare more humanistic, and that you can’t solve a problem with the same thinking that created it. In the “roadmap” Zeev shows how we must employ marketing principles such as branding, segmentation, and process design from the perspective of the customer, if we are going to make a difference. He suggests that these tools may have as much or more to offer us as does payment reform, clinical redesign, or the further development of digital tools. His core objective is to humanize healthcare. He is convinced that “…value is locked up in the system and needs to be liberated.” The ultimate objective of reframing healthcare is to save lives.
I was delighted to see that Zeev’s concepts culminate in the discussion of how to address the “social determinants of health.” He begins the chapter before his epilogue by going back to the 2007 New England Journal article, “We Can Do Better–Improving the Health of America” by Stephen Schroder. He first pointed out Schroder’s article to me early in 2008. He had lifted a slide from the article which he explained to me and gave me. I have used that slide in the majority of talks that I have ever given since, and you have seen it in these notes before. Here it is again.
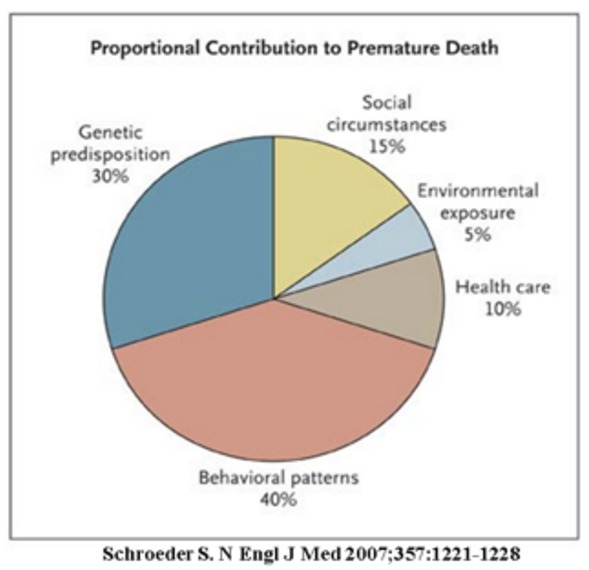
Zeev used the article and the slide to point out to me then that we needed to focus on issues that are much broader than we were currently addressing in our practice. He is still pushing that enlightening observation. He writes:
Approximately 60 percent of our health outcomes are determined by social causes while only 10 to 20 percent are due to what we consider our healthcare delivery system.
He goes on to reiterate something else that we all know, but do not know how to address:
One’s ZIP code is a better predictor of health and longevity than one’s genetic code.
Zeev points out that the negative realities that are driven by the inequities that constitute the social determinants of health and emphasizes our neglect of these concerns. The consequences of ineffectively addressing the social determinants of health are born by all of us through their impact on the cost structure of healthcare. He references the 2016 book, Poverty and the Myths of Health Care Reform, written by Richard Cooper, MD which reports that ED visits and hospitalization rates are inversely related to income while poor health outcomes are directly proportional to low incomes. If we are trying to achieve Triple Aim goals without addressing poverty and the social determinants of health, we are on a fool’s errand. To support our logical approach to improving the health and the healthcare care of those living with poverty, Zeev offers the Health Prioritization Protocol (HPP).
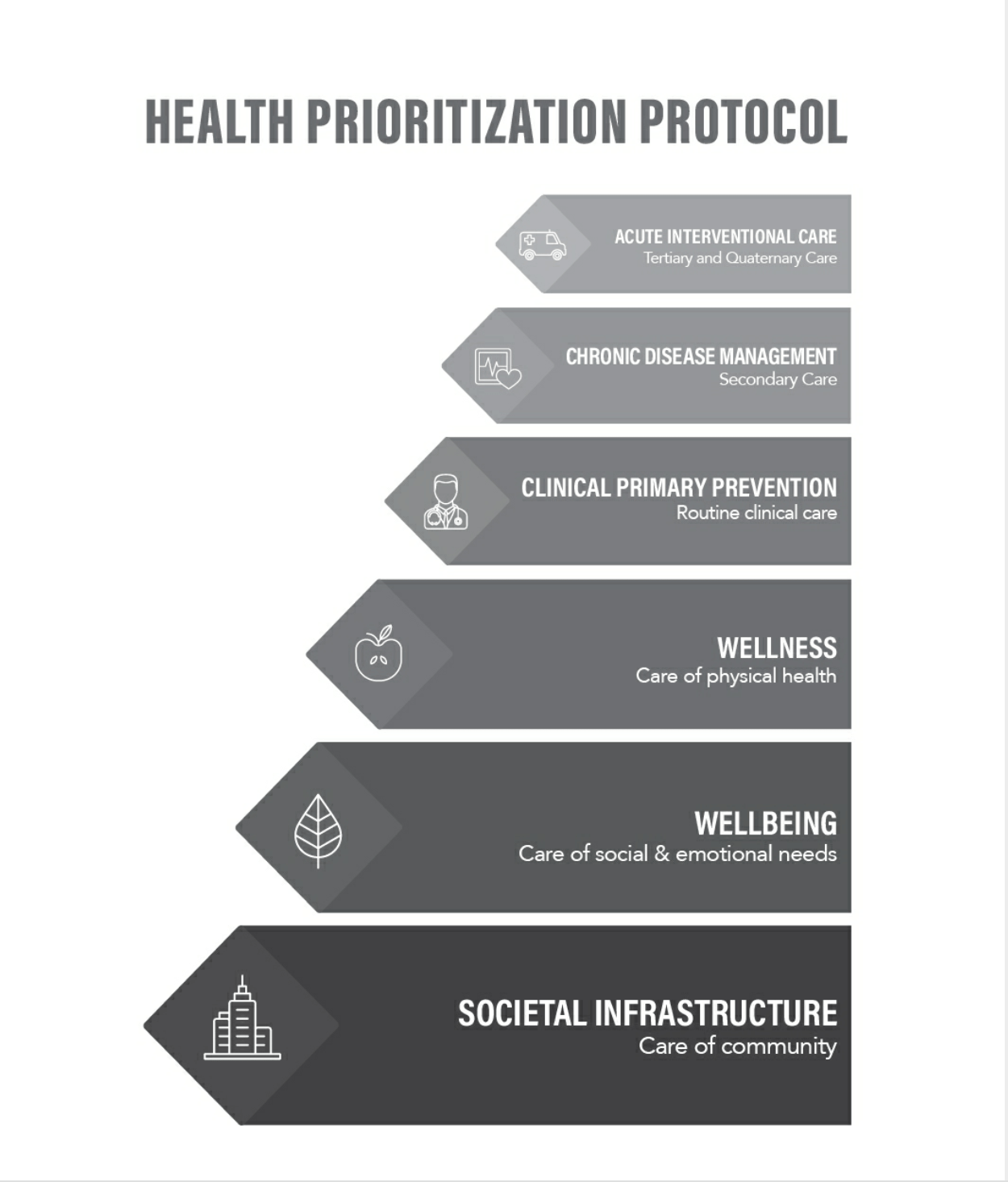
In the graphic he presents a logical six step analysis of how to effectively address the social determinants of health. He states:
We as a nation, need a more explicit, standardized, and systematic way to prioritize our attention, our strategies, and our resources on the social determinants of health.
Here is the explanation of the logic of the graphic:
- The foundational step is social infrastructure: shelter; clothing; healthful food; safe air, water, and soil; safe stable neighborhoods and communities; convenient access to affordable transportation; and the ability to gather socially. He states that the most impactful elements on healthcare are education, employment, and income.
- Wellbeing: “interpersonal infrastructure,” that which encompasses one’s emotional, relational, and social life and how one is connected to others in the community. “It’s about how much control, mastery, and autonomy and resilience one has…to face life’s challenges.”
- Wellness: Physical well-being: nutrition, physical activity and movement, sleep hygiene, the avoidance of toxins like tobacco, excessive alcohol, and opiates.
- Clinical Primary Prevention: Disease screening, genetic testing, dental care, immunizations
- Chronic disease management: Secondary prevention, maintaining health as optimally as possible despite existing medical conditions. Chronic disease management now represents the vast majority of healthcare encounters which means that it “represents the greatest immediate and most proximal opportunity for improving health and reducing avoidable costs.
Let me interject here, before giving the last bullet point, that Zeev implies the obvious fact that effective attention to the first four objectives greatly reduces the number and severity of those suffering from chronic disease and acute illness. The dividend to society from investing in societal infrastructure, well-being, wellness, and clinical primary prevention is enormous and goes beyond just the reduction in terms of lower costs for chronic disease and care acute management. Those investments should also reduce our costs for crime prevention, enable efforts directed against violence and domestic abuse, provide us with a better equipped and more productive workforce, while reducing demands for chromic care and emergence medical and social services.
The final level in the pyramid of Zeev’s Health Prioritization Protocol is:
- Acute Care: This is where we spend the most dollars with the least impact on health. It includes high cost, high tech diagnostic and surgical interventions and other complex hospital based care. The volume, intensity, and cost of the services needed in this category are inversely related to our attention and investments in the other five steps. We focus our efforts here when we rely on fee for service payment and maximizing the volume of work that must be done to earn the revenue that supports the infrastructure that we have created. Inappropriate utilization becomes the covert strategy for success.
Zeev addresses with practical advice and observations from work at Geisinger Clinic how to shift our emphasis and transition our resources to bring effective attention to the first three foundational steps of the HPP. I will surely be returning to his insights in future posts. A commonly used metaphor in healthcare policy conversations these days pictures us in the precarious position of having one foot in a “tippy” canoe and the other foot on a sinking dock. Zeev’s book is sound advice for any healthcare leader who can understand the sense of imbalance, confusion, and jeopardy that the metaphor implies.
His book should also be a relief for those on the frontlines of care delivery who suffer daily from the necessity of trying to help people while working in organizations that keep trying to solve today’s problems with the same thinking and principles that created our current dilemma. For me it was like a letter from an old friend whose positive outlook, enthusiasm for our work, and compassion for everyone has always been an inspiration and a source of hope. I give Zeev a huge “thank you” for his many continuing efforts and the gift of this book. I give you the recommendation that if you care about health, healthcare, and your community, you need to start reading this book today.
